The ESTRO 2024 closing debate saw speakers discuss whether the radiation therapy care pathway will be delivered entirely by bots by 2040

The closing debate of the ESTRO congress always serves to both educate and entertain, and ESTRO 2024 was no exception. Billed as “Clash of the tartans – the great AI debate” – in a nod to this year’s Glasgow location, the presenters debated the motion: “This house believes that the radiation therapy care pathway will be delivered entirely by bots by 2040”.
“The only way forward”
The first speaker, Andrew Hope from the Princess Margaret Cancer Center in Toronto, explained that population growth is leading to an insurmountable cancer burden, with worldwide cancer cases predicted to roughly double by 2040. He argued that, with hospitals already struggling to meet the demands of cancer patients, automation is the only possible way forward.
Hope described how the immense amount of computational power now at our disposal is being applied to new applications such as artificial intelligence (AI). “Just in the last five years we have gone from relatively simple games like AlphaGo to real functional applications that affect our day-to-day life,” he explained.
Alongside, AI-based robotics – machines that translate computational power into the physical world – have progressed at vast pace. Within industry and manufacturing, robotics is becoming an absolute necessity, Hope explained. “This is happening whether we like it or not, which is why we need to adapt it and incorporate bots and automation into healthcare immediately.”
In many ways, we already have. AI is now being developed for every step stage in the radiotherapy care pathway – from diagnostic imaging to treatment planning and delivery to follow-up. The only thing that’s not yet being done is to look at this as a cohesive whole and run it without significant human intervention.
“It doesn’t mean we’re all out of jobs,” Hope added. “It just means we get to do more of what we love, which is talking to patients and addressing their concerns, adjudicating challenging cases and improving the bots to make this entire pathway more seamless, safe and flexible.”
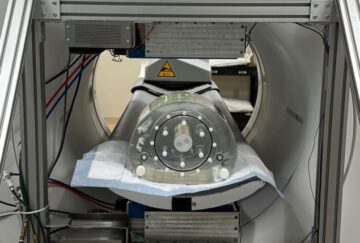
He shared an example of a next-generation treatment system that can scan, plan and treat in one, using two robot arms, one housing the detector and the other the treatment and diagnostic unit. The system can move around a patient to capture a cone-beam CT, then immediately plan, contour and treat with the patient still in place.
“We can automate, and we should, because we have to,” Hope concluded. “We have to treat people rapidly, and safely. Even if we become a virtual automated hospital, it’s still going to be something that we can control.”

“AI is stupid”
Andre Dekker, a medical physicist at MAASTRO Clinic, does not agree. He began his presentation by explaining how Croatia has the toughest conditions in the world for acquiring a driving license, requiring 85 hours of lessons before even taking a driving test. So why not move to a self-driving car instead? He pointed out that Google started its project on self-driving cars 15 years ago, but today there’s still no truly autonomous vehicle on the market.
And while it takes 85 hours to get a driving license in Croatia, it requires 11 years of education to train as a radiation oncologist, physicist or radiation therapist (RTT). “The assumption that in 15 years we can automate the entire radiation oncology pathway is just ludicrous. It’s never going to happen. We cannot automate 11 years of specialized education.”
Dekker’s second argument was simply that “AI is stupid”. When analysing images, for example, humans can recognise related features via “few shot learning”, which AI simply cannot do. AI trained to identify the liver in a supine CT scan, for example, can’t recognize a liver in a prone scan, whereas a human could. “AI is so stupid if you give it a scan of the head it will draw you a liver,” he said. “AI will make mistakes that harm patients.”

A glimpse into the future of radiation therapy
AI is also biased, Dekker said, sharing a photo of two female colleagues, both physicists, in a kayak in Michigan. He then asked AI to generate an image of “two physicists in a kayak in Michigan” – it drew two old white men with grey beards. This bias could prove even more problematic in healthcare. “AI-based bots will not give equally good care to everyone,” he said, noting that it is particularly unsuitable for use in low- and middle-income countries.
“AI will not replace us,” Dekker emphasized. “I don’t believe that the entire radiotherapy care pathway will be taken over by bots, because AI will not be ready for it in 15 years, AI cannot handle new things that humans can do much better. AI will be biased and tell you only things you already knew or that are fake. Don’t believe in it.”
“Can we, should we, will we?”
Next up, Stine Korreman from Aarhus University pointed out that in this year’s ESTRO programme, every single time slot could be covered with a presentation on AI. She cited one poster discussion demonstrating fully automated radiotherapy treatment planning, from scan to plan. “If we are able to do this now, where will be in 2040?”
Korreman demonstrated a foundation model performing real-time image delineation. “This is not trained for this specific purpose, this is just plug-and-play,” she said. “By 2040 AI will have the capability to process all data, all the time, everywhere. This is something humans are not able to do.”
So just because we can, should we? Korreman said that many problems attributed to AI – automation bias, overreliance, overcompliance and so on – are actually related to the humans using the AI. Showing a delineation error made by AI due to different patient positioning, she noted: “I can tell you exactly why it made that mistake and I can retrain and fix the model”. But if a human makes a delineation error, we’ll often have no idea why they did that or how to fix it. “The human brain is a black box more than an AI model,” she emphasized.

Bridging the knowledge gap on AI and machine-learning technologies
Returning to the car analogy, Korreman pointed out that any accident involving a self-driving vehicle is big news. But statistics show that accidents occur far more often in human-driven vehicles, and that most accidents involving self-driving vehicles are actually caused by the human driver it met. “This is a very good reason to go in that direction. You may say AI is stupid, but humans driving cars can be really stupid.”
So yes, we should. But will we? Korreman suggested that today’s ESTRO delegates will not, citing a survey from a pre-meeting course in which 72% thought that radiotherapy cannot totally move to AI-based automation – human oversight will be needed at some key steps. Rather, she said, it will be the younger generation, who are already at ease with AI-based applications, who will drive this. “This will happen, not by us, but by a new generation of people who are not afraid of breaking barriers.”
“Humans are here to stay”
Finally, Eliana Vasquez Osorio from the University of Manchester argued against the motion. She pointed out that the conversation so far was all about treatment optimization and delivery, but the care pathway also includes treatment decision and patient follow-up stages, which involve a large multidisciplinary team.
“None of my esteemed colleagues have been able to actually say that the whole human team is going to be replaced; humans are there and we are going to keep them,” she said. To investigate this further, Vasquez Osorio conferred with various people currently performing patient treatments to understand where and how bots could replace them.
Vasquez Osorio spoke to an oncologist about the “walk into the clinic test”. A patient’s data may indicate use of a standard chemoradiotherapy regime, for example. But then the oncologist sees the patient struggling to walk and decides that this approach is too aggressive. They will talk with the patient, discuss the case with the multidisciplinary team, and integrate all this information to select the final treatment course.
A bot will just use the data to choose a treatment, with no input from the patient and no extra information available.
For a complex reirradiation case, the oncologist may be tasked with deciding between recommending palliative or radical treatment. With the bot, “computer says no,” said Vasquez Osorio. “This speciality will not be replaced by any kind of bot.”

How to train the medical physicists of the future
Then there’s the medical physicist, who has many responsibilities, including safety-critical tasks such as quality assurance. Vasquez Osorio described the case of the MCAS flight stabilizing system that, when triggered by a faulty sensor, led to two fatal plane accidents. “We can learn from other disciplines,” she said. “Medical physicists are not going to be replaced by bots.”
Finally, the RTTs talk to the patients each day, noticing any deterioration and triggering appropriate interventions. “The RTTs are empathetic, genuine and non-judgemental,” Vasquez Osorio pointed out. “You are not going to open up your heart to a bot, so you lose extra information.”
Vasquez Osorio explained that a patient’s perception of treatment, and whether they feel it is in their best interest, is connected to building trust with the clinicians. She cited a patient representative who told her: “bots are akin to the patient being on a conveyor belt, treatment is ‘done to them’ not ‘for them’”.
“The question becomes whether an exclusively bot-driven care pathway is best for the patients,” she concluded.

At the close of the session, the motion was opened for an audience vote (with a can of Irn-Bru up for grabs by the winners). The ESTRO delegates voted 83% against the motion – perhaps echoing Korreman’s prediction that “this will happen, but not by us”.
- SEO Powered Content & PR Distribution. Get Amplified Today.
- PlatoData.Network Vertical Generative Ai. Empower Yourself. Access Here.
- PlatoAiStream. Web3 Intelligence. Knowledge Amplified. Access Here.
- PlatoESG. Carbon, CleanTech, Energy, Environment, Solar, Waste Management. Access Here.
- PlatoHealth. Biotech and Clinical Trials Intelligence. Access Here.
- Source: https://physicsworld.com/a/will-future-radiotherapy-be-delivered-entirely-by-ai-bots/
- :has
- :is
- :not
- :where
- $UP
- 11
- 120
- 15 years
- 15%
- 2024
- 2040
- 90
- a
- Able
- About
- Absolute
- accident
- accidents
- acquiring
- actually
- adapt
- added
- addressing
- affect
- afraid
- against
- aggressive
- ago
- agree
- AI
- AI bots
- All
- already
- also
- always
- amount
- an
- analysing
- and
- andre
- anna
- any
- applications
- applied
- approach
- appropriate
- ARE
- argued
- argument
- arms
- around
- artificial
- artificial intelligence
- Artificial intelligence (AI)
- AS
- asked
- assumption
- assurance
- At
- audience
- automate
- Automated
- Automation
- autonomous
- autonomous vehicle
- available
- barriers
- BE
- because
- become
- becomes
- becoming
- been
- before
- began
- being
- believe
- believes
- BEST
- Better
- between
- bias
- biased
- Big
- billed
- Black
- Bot
- both
- bots
- Box
- Brain
- Breaking
- Building
- burden
- but
- by
- CAN
- Cancer
- cancer patients
- cannot
- capability
- capture
- car
- care
- cars
- case
- cases
- caused
- Center
- centre
- Chair
- challenging
- Choose
- cited
- citing
- click
- clinic
- clinicians
- Close
- closing
- cohesive
- colleagues
- complex
- computational
- computational power
- Concerns
- concluded
- conditions
- conferred
- Congress
- connected
- control
- Conversation
- could
- countries
- course
- courtesy
- covered
- Croatia
- Currently
- data
- day
- day-to-day
- debate
- debated
- Deciding
- decision
- delegates
- delivered
- delivery
- demands
- demonstrated
- demonstrating
- described
- developed
- diagnostic
- Diagnostic imaging
- DID
- different
- direction
- disciplines
- discuss
- discussion
- disposal
- do
- does
- Doesn’t
- done
- Dont
- double
- draw
- drive
- driver
- driving
- due
- each
- ease
- echoing
- educate
- Education
- emphasized
- enough
- entertain
- Entire
- entirely
- equally
- error
- esteemed
- Ether (ETH)
- Even
- Every
- everyone
- everywhere
- exactly
- example
- exception
- exclusively
- explained
- explaining
- extra
- fake
- far
- faulty
- Features
- feel
- female
- final
- First
- five
- Fix
- flexible
- flight
- For
- Forward
- Foundation
- from
- fully
- functional
- further
- future
- Games
- gap
- generate
- generation
- genuine
- get
- Give
- Glimpse
- Go
- going
- gone
- good
- great
- Growth
- handle
- happen
- Happening
- harm
- Have
- he
- head
- healthcare
- Heart
- her
- here
- High
- his
- hope
- Hospital
- hospitals
- HOURS
- House
- housing
- How
- How To
- HTTPS
- human
- Humans
- i
- idea
- identify
- if
- image
- images
- Imaging
- immediately
- immense
- improving
- in
- includes
- Including
- incorporate
- indicate
- industry
- information
- input
- instead
- integrate
- Intelligence
- interest
- intervention
- interventions
- into
- investigate
- involve
- involving
- issue
- IT
- ITS
- Jobs
- jpg
- just
- Keep
- Key
- Kind
- kirby
- knew
- knowledge
- large
- Last
- leading
- LEARN
- Led
- Lessons
- License
- Life
- like
- Liver
- location
- Look
- lose
- love
- Machines
- made
- make
- MAKES
- manchester
- manufacturing
- many
- Market
- max-width
- May..
- mean
- means
- medical
- Meet
- Men
- met
- Michigan
- mistake
- mistakes
- model
- more
- most
- motion
- move
- much
- multidisciplinary
- my
- necessity
- Need
- needed
- never
- New
- news
- next-generation
- no
- noted
- noting
- now
- occur
- of
- often
- Old
- on
- oncology
- ONE
- only
- open
- opened
- optimization
- or
- Other
- our
- out
- over
- Oversight
- Pace
- particularly
- pathway
- patient
- patients
- People
- perception
- performing
- perhaps
- photo
- physical
- physicist
- Physics
- Physics World
- Place
- plan
- plane
- planning
- plato
- Plato Data Intelligence
- PlatoData
- population
- positioning
- possible
- poster
- power
- predicted
- prediction
- presentation
- presents
- prize
- problems
- process
- programme
- progressed
- project
- Prove
- purpose
- quality
- question
- Radiation
- radical
- Radiotherapy
- rapidly
- rather
- ready
- real
- real-time
- really
- reason
- recognise
- recognize
- recommending
- regime
- related
- relatively
- replace
- replaced
- representative
- requires
- responsibilities
- robot
- robotics
- roughly
- Run
- safe
- safely
- Said
- saw
- say
- says
- scan
- seamless
- Second
- sees
- select
- self-driving
- self-driving car
- self-driving vehicles
- serves
- session
- shared
- sharing
- she
- shot
- should
- show
- showing
- significant
- Simple
- simply
- single
- slot
- So
- so Far
- some
- something
- Speaker
- speakers
- specialized
- specific
- Stage
- stages
- standard
- started
- statistics
- stay
- Step
- Steps
- Still
- Struggling
- such
- Survey
- system
- taken
- takes
- taking
- Talk
- talking
- tasked
- tasks
- team
- tell
- test
- than
- that
- The
- The Future
- the world
- their
- Them
- then
- therapist
- therapy
- There.
- they
- thing
- things
- this
- thought
- thumbnail
- time
- to
- today
- today’s
- told
- too
- toronto
- TOTALLY
- Train
- trained
- translate
- treat
- treatment
- treatments
- triggered
- triggering
- true
- truly
- Trust
- two
- Ultimately
- understand
- unit
- university
- us
- use
- using
- various
- Vast
- vehicle
- Vehicles
- very
- via
- Virtual
- Virtual Automated
- Vote
- voted
- walk
- was
- Way..
- ways
- we
- What
- when
- whereas
- whether
- which
- while
- white
- WHO
- whole
- why
- Wikipedia
- will
- winners
- with
- within
- without
- world
- worldwide
- years
- yes
- yet
- you
- Younger
- Your
- zephyrnet